
CY 2027 Risk Adjustment, made operational.
Every year CMS tells Medicare Advantage plans how they'll get paid for the health of their members. For CY 2027, most of the machine stays the same — but two new rules quietly change which diagnoses count, and both land mid-year instead of in January. Here's what's changing, when it bites, and what your team should do before July 2027.
Reference: CMS HPMS memo, "Calendar Year (CY) 2027 Risk Adjustment Implementation Information," July 9, 2026
The quick map: 2 new rules · 3 model runs · 1 report you can't ignore · 0 changes to the models
First, one word that confuses everyone: "CY"
CY 2027 = the year you get paid, not the year the diagnoses come from.
Read "CY 2027" as payment year 2027 — January through December 2027. The clinical data feeding those payments is older, from 2025 and 2026 dates of service. CMS says it plainly: the new audio-only rule applies "for payment year 2027 (2026 dates of service)."
Lock that in and the rest of the memo reads easily: CY 2027 is when the money moves; the diagnoses behind it are a year or two old.
The headline: CMS is tightening what counts as a real diagnosis
Two categories of "easy" diagnoses are getting cut off. Both share one theme — prove it's real, or it doesn't count — and both wait until the Midyear run (~July 2027) to take effect.
Rule 1 — Phone-only visits stop counting
Diagnoses from audio-only telehealth (a phone call, no video) will be excluded. CMS's logic, stated plainly in the memo: diagnoses must result from face-to-face encounters to count for risk adjustment.
How they spot it: the "93" or "FQ" modifier on the record.
Where it applies: professional and outpatient encounter data, chart review records, and FFS claims — both PACE and non-PACE, every provider type.
The safety valve: the diagnoses only drop if every risk-adjustment-eligible line item on the record carries a 93 or FQ modifier. If even one eligible line lacks it, all the header diagnoses still count.
Your move: clean modifier use and provider education. Sloppy coding here can quietly cost you valid diagnoses.
Rule 2 — Chart reviews that can't be linked stop counting
A chart review record (CRR) is a diagnosis your team pulled from a member's chart. New rule: if you can't link it back to a real original encounter, CMS throws it out. Non-PACE only.
The one exception: if the member switched from an MA contract in one parent organization to a contract in a different parent organization, unlinked CRR diagnoses stay valid. CMS checks by comparing the parent org on the date of service against the parent org at submission.
Why this is the big one: it puts a dollar value on your ability to trace a chart diagnosis back to a real encounter. Link it and you keep the money. Can't link it and you watch it vanish at Midyear. This is a data-integrity problem you want solved well before July 2027.
So — does a given diagnosis still count?
Once both exclusions are live, every diagnosis runs the same gauntlet. Here's the whole test in one picture:
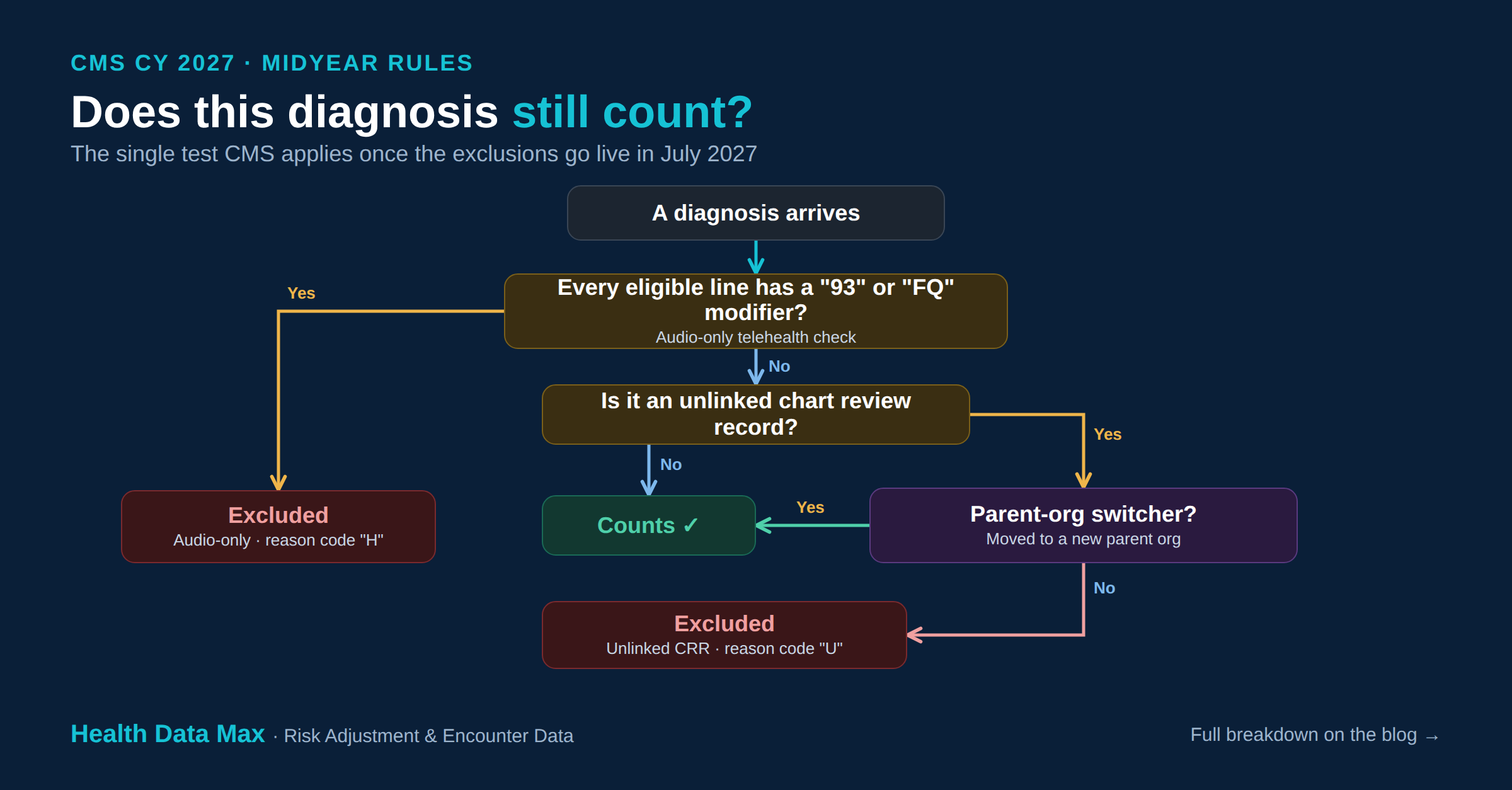
Three possible outcomes — it counts, or it drops out one of two ways. Audio-only exclusions land under the existing code "H." Unlinked-CRR exclusions get a brand-new code "U."
Don't blur the scope: the audio-only rule hits everyone — PACE and non-PACE alike. The unlinked-CRR rule hits non-PACE only. Two rules, two different blast radii.
The timing: your first-half 2027 payments are only a draft
Same payment year, three runs. The two new rules only apply to runs two and three — so early payments get reworked later.
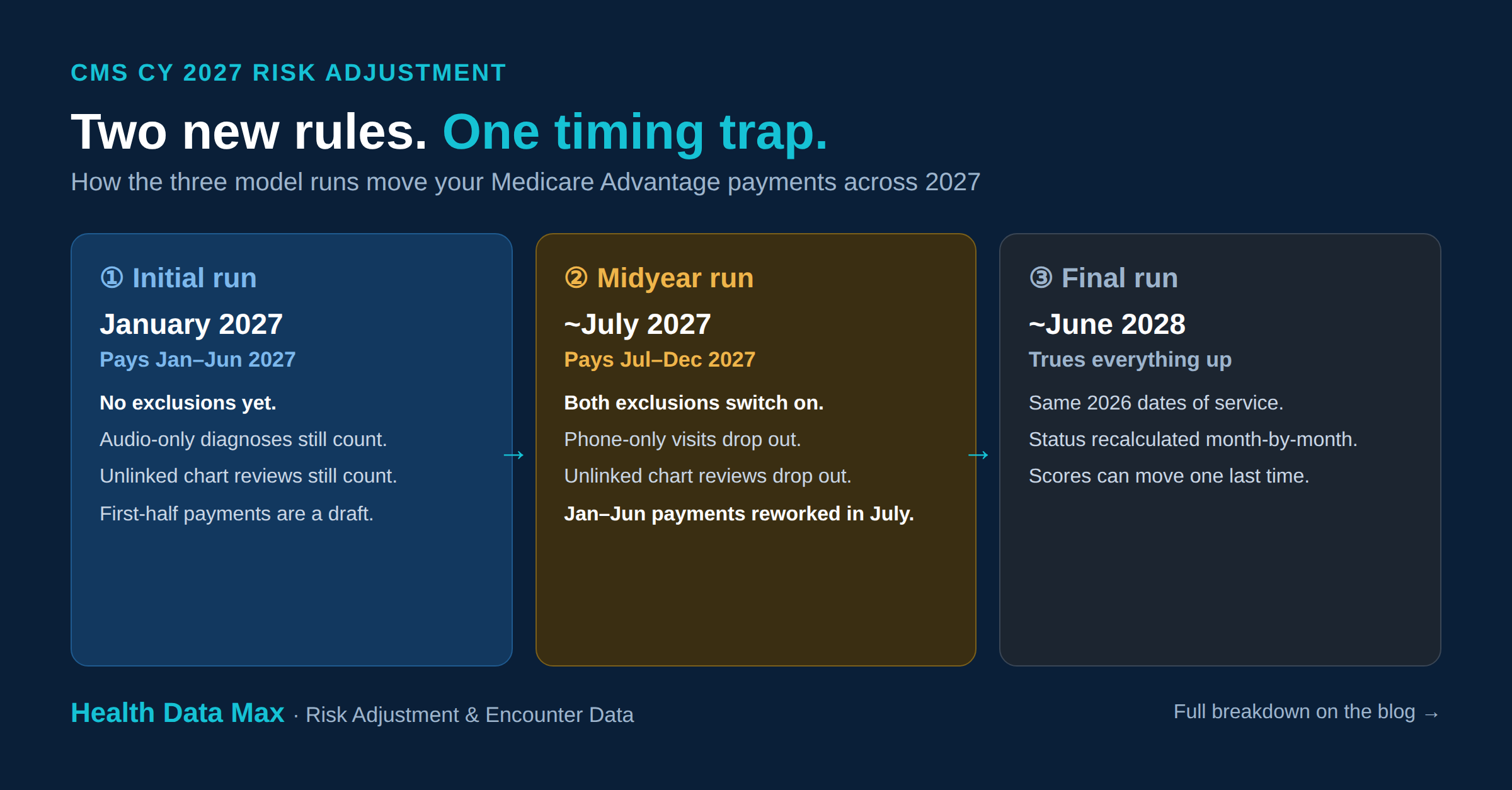
① Initial run — pays Jan–Jun 2027
No exclusions yet. Everything still counts. Scores use Jul 2025–Jun 2026 dates of service.
② Midyear run (~July 2027) — pays Jul–Dec 2027
Both exclusions switch on. Scores shift to full-year 2026 dates of service. And your Jan–Jun payments get retroactively adjusted in July.
③ Final run (~June 2028) — trues everything up
Same 2026 data as Midyear, but member status is recalculated month-by-month, so scores can move one more time.
The takeaway: don't treat January–June 2027 payments as final. They're calculated under the loose rules, then reworked under the strict ones in July. Forecast conservatively.
The report that trips people up: MAO-004
This is where reconciliation quietly breaks. The MAO-004 tells you which diagnoses CMS allowed or rejected — and it's changing.
New Reason Code "U" → flags an unlinked-CRR diagnosis that didn't qualify for the switcher exception.
Audio-only reuses existing Code "H" → no new code for that one.
The trap: for submission months Jan–Sep 2026, you get two versions of the report — the original (no exclusions) and a November 2026 reissue (with exclusions). They disagree by design. From October 2026 submissions onward, the report reflects the exclusions natively.
Your move: make sure whoever owns MAO-004 knows which version maps to which run — before November 2026 lands.
What's NOT changing (so nobody over-prepares)
Plenty is staying put:
Models: non-PACE continues on the 2024 CMS-HCC model (V28) and the 2023 ESRD model (V24) — the memo describes no blending for non-PACE. PACE keeps its 50/50 blends across CMS-HCC, ESRD, and RxHCC.
MMR: no updates at all.
MORs: no new record types — the RxHCC types 6 and 7 carry over.
Two more things to load in
New normalization factors. Fresh numbers to configure for 2027 payment: 2024 CMS-HCC = 1.079, 2017 model = 1.202, and a split RxHCC of 1.109 (MA-PD) / 1.005 (PDP). (These keep average scores anchored near 1.0 so coding intensity doesn't inflate payments.)
SAS is retiring. Both SAS and Python are offered for CY 2027 — but CY 2028 is Python-only. If your tooling runs on SAS, 2027 is your runway. Don't wait.
One line to keep straight: this is Medicare Advantage, not ACA
This memo is the MA pipeline — MMR, MAO-004, MORs, encounter-data-to-HCC. It's a completely separate system from the ACA/Marketplace EDGE server world. Same "risk adjustment" words, different plumbing. If one team touches both, don't cross the wires.
The bottom line
CMS is raising the bar on proof. Phone-only visits and chart reviews you can't link stop paying at Midyear 2027. For an operations or compliance leader, that's a short list:
Fix your chart-linking — unlinked diagnoses are about to lose their value.
Audit audio-only modifiers and educate providers.
Prep MAO-004 reconciliation for the dual-report reissue.
Forecast conservatively for Jan–Jun 2027; it gets adjusted in July.
Start your SAS-to-Python migration before 2028 forces it.
Everything else is continuity. The work lives in data integrity and timing — get those two right and CY 2027 is a smooth year.